Pain Regimen
https://www.youtube.com/watch?v=06OISvbIhTA&list=PLt6NrpvPjCbKJ7PXXzrmZ2s4U9CUGroPE&index=40
Brief overview of some of the treatment options available to you when a patient is in the hospital and complaining of pain.
Acetaminophen (Tylenol)
- Typical dosing: 650mg q4h prn or 1000mg q6hr prn
- Max 4g/day in typical patients, max 2g/day in patients with cirrhosis / liver dysfunction
- I basically put every patient on prn tylenol on admission
- Toxicity isn't usually seen until about 10 grams of tylenol in one day
- Also referred to as APAP by some people (N-acetyl-para-aminophenol) - I think sticking with tylenol or acetaminophen is better: APAP: An Error Prone Abbreviation
- Consider scheduled doses in patients with uncontrolled pain
- Oral or rectal are good routes. IV is good but pharmacy doesn't like you using it too much because it is expensive.
NSAIDs
- Make sure patient is not at risk of GI bleed or has an AKI. Not commonly used for inpatients due to these risks.
- Ibuprofen (MOTRIN, ADVIL) - 400-600mg PO every 6-8 hrs
- I like 400mg because the evidence seems to show it has the same analgesic effect and as you go higher you only increase the risk of side effects.
- Naproxen (ALEVE) - can be dosed every 12 hours. Higher risk of GI bleed
- Ketorolac (TORADOL) - IV/IM forms available which can be useful especially in patients with nausea. Useful in kidney stones. Highest rate of GI bleed though debatable. 10-15mg is equivalent to 30mg in terms of pain relief. Q6h x48 hours is an appropriate trial in setting of acute pain, after that can transition to celecoxib to reduce the risk of GI bleed or renal issues (200mg BID)
- Indomethacin - commonly used in gout, 50mg TID during flare. For general treatment of pain, 20mg TID (I don't see this inpatient much if ever).
- Celecoxib (CELEBREX) - newer evidence does not show increased risk of heart attacks / ischemic cardiovascular events. May have lower risk of GI bleed (Chan, et al 2017). Might start seeing this used more going forward.
Lidocaine patch
- Good for musculoskeletal pain
- Up to 3 patches
- Placed and removed every 24 hours
- 5% form is hard to get outpatient due to insurance coverage issues but there are OTC 2% and 4% forms
Capsaicin cream
- Some patients like it, others don't like the burning feeling
- Binds to nociceptors in the skin -> initial excitation and enhanced sensitivity -> followed by refractory period with reduced sensitivity and persistent desensitization, possibly due to depletion of substance P
- Most effective for osteoarthritis (0.025% cream), neuropathic pain (0.075% cream, not available at our hospital), and cancer-related pain
- Double-blind trial showing 80% of patients with osteoarthritis had reduced pain after 2 weeks: https://pubmed.ncbi.nlm.nih.gov/1954640/
- Efficacious, but moderate to poor efficacy: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC404499/
- High reports of burning/redness, but patients liked it and continued to take it due to decreased neuropathic pain: https://pubmed.ncbi.nlm.nih.gov/9256142/
Diclofenac gel (VOLTAREN gel)
- 1% gel up to 4 times daily
- Often used in osteoarthritis
- 3% gel is for actinic keratosis not for pain
- Low systemic absorption so avoids most of the side effects of NSAIDs
Opioids
-
Tramadol
- Partial mu and serotonin receptor agonist, "dirty" as it hits a lot of different receptors
- Falling out of favor as patients have very different responses
- Side effect = lowered seizure threshold
- 50mg q4-6hr prn
-
Oxycodone
- Commonly start with 5mg dose in patients, 2.5mg if elderly
- Onset in 10-30 minutes and lasts 3-6 hours
- Extended release version = OXYCONTIN (lasts for 12 hours)
-
Hydromorphone (DILAUDID)
- The reasons patients like it is because it has a more rapid onset of analgesia which can produce more euphoria
- Metabolized by LIVER (don't give in liver dysfunction!)
-
Morphine
- Good for air hunger, decreasing anxiety
- Frequently seen in patients on hospice or comfort care
- Has a liquid version called ROXANOL
- Has an extended version called MS-CONTIN
- Metabolized by KIDNEY (don't give in kidney dysfunction!)
-
Meperidine (DEMEROL)
- Thought to be good in pancreatitis due to decreased contraction of Sphincter of Oddi
- Useful in patients with rigors
-
Miscellaneous
- Common outpatient meds - hydrocodone-acetaminophen (NORCO), oxycodone-acetaminophen (PERCOCET, VICODIN). Can continue this when inpatient though typically we do prefer to separate the oxycodone and acetaminophen from each other to optimize dosing
- Make sure everyone on opioids has opioid overdose order set (includes naloxone for reversal if needed)
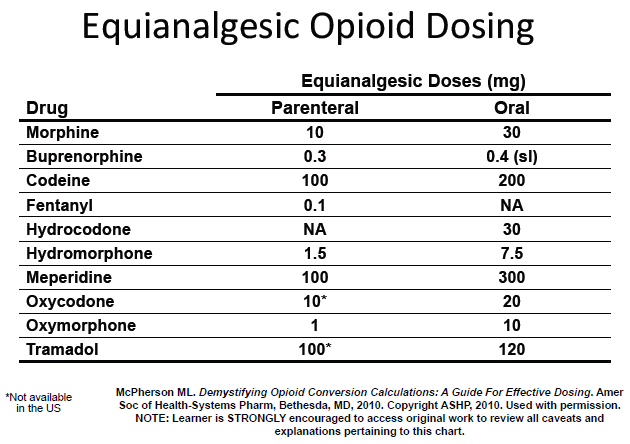
Make sure everyone on opioids has a solid bowel regimen (at least miralax and senna)! Constipation common - USE THE CONVERSION CHART TO SEE DOSING EQUIVALENTS
- When switching from one opioid you may want to consider initially dose reducing about 75% to account for differences in pharmacokinetics
Neuropathic pain treatments
- Remember neuropathic pain vs nociceptive pain. Neuropathic pain does not respond well to opioids.
- Duloxetine (CYMBALTA)
- Venlafaxine (EFFEXOR)
- Gabapentin (NEURONTIN)
- TCAs are also used for this but very unlikely would be started inpatient, lots of side effects
Methadone
- Used in patients who are trying to wean off opioids - long-acting
- IV AND PO methadone has QT prolongation which you should be wary about, get pain management involved
- If coming in with acute pain, switch from daily dosing to TID as analgesic effect is only about 6-8 hours
- Useful in palliative setting
- Good for patients with absorption issues (85% bioavailable and predominantly absorbed in the stomach)
- Has some benefits for neuropathic pain as well
Ketamine
- Consult pain pharmacy if considering to start this
- Gaining popularity as an opioid-sparing pain medication
- Has some dissociation as a side effect which can actually be beneficial in pain
- Side effects = emergence reactions, hallucinations
Buprenorphine
- Also gaining popularity
- Partial agonist of mu receptor - meaning it acts as an agonist when there's no opioid around. But when there is opioid around it becomes an ANTAGONIST so it prevents people from doing opioids on top of their prescribed pain meds
- Has a lower risk of respiratory depression compared to traditional opioids
Miscellaneous
- Lidocaine swish & swallow - for mouth pain / ulcers
- Lidocaine gel (URO-JET) - for painful Foleys
- Warm compress (K-PAD) - for pain related to localized swelling
- Muscle relaxants - baclofen, cyclobenzaprine, tizanidine, etc. - they all basically work just by making you sedated and sleepy from what I learned. Doesn't really actually do that much for pain. Baclofen really should only be used for central spastic disease, it's not a great drug, also watch out for baclofen withdrawal in admitted patients (looks kind of like alcohol withdrawal, risk of seizures, etc.)
- Long-acting vs short-acting opioids - you shouldn't really ever use long-acting narcotics in the standard patient population. They have high abuse and overdose potential and don't really work well for most acute or chronic pain issues. Their role is really in pain related to cancer or end-of-life related pain. In cancer patients you often will see them combined with short acting in a manner similar to basal-bolus insulin regimens. Per /u/Dominus_Anulorum
- Don't forget to make use of consult services
- Pain pharmacy consult
- Wound care consult
Post-operative pain control
- Per u/MMOSurgeon , read more comprehensive post here
- For midline, subcostal, Chevron, or Mercedes incisions - thoracic epidural is the gold standard
- Standing tylenol is important!
- Toradol is an excellent choice, also order it standing
- Oral medications ALWAYS WORK BETTER AND LAST LONGER than IV pushes or PCAs
- Consider regional blocks
- Read the guide from Michigan for discharge to home / how many opioids to send a patient home on





{kind=link}